
Summary
1.1. Summary of key concepts and guidelines (ANZCOR 2021)
Irrespective of the presence or absence of antenatal or intrapartum risk factors, the need for resuscitation should always be anticipated. Equipment and personnel trained in newborn resuscitation should be available at all births. At least one person should be responsible for the care of each newborn.
Evaluating the need to initiate and continue resuscitation should begin immediately at birth and proceed throughout the resuscitation. Initial assessment is based on three questions:
- Is the infant term gestation
- Is the infant breathing or crying?
- Does the infant have good muscle tone?
Newly born infants of any gestation who are floppy, not moving and/or not breathing or crying at birth should be promptly transferred to the resuscitaire for assessment. First response interventions are indicated. Advanced resuscitation interventions may be required.
Preterm infants are at particular risk of hypothermia. Following birth, attention to preventing hypothermia in addition to assessing tone, breathing effort and heart rate is paramount. Very preterm infants <32 weeks’ gestation, and especially those <28 weeks’ gestation or <1500 g birth weight should be placed immediately into a polyethylene bag or wrap while still wet and warm, and placed under a radiant heat source on the resuscitaire for further assessment. More mature preterm infants should be dried and assessed on the resuscitaire.
A term or near term infant who cries, moves and assumes a flexed posture after birth is unlikely to require resuscitation. These infants can be placed skin-to-skin on their mother’s chest or abdomen while simple interventions such as drying, providing warmth and clearing the airway (only if necessary) are performed. An uncompromised infant should breathe effectively and their heart rate should rise rapidly above 100 beats per minute. If this does not occur following a brief period of stimulation (not more than 20 seconds) the infant should be transferred to the resuscitaire for further assessment. First response interventions are now indicated.
First Response Interventions:
First response interventions focus on airway, breathing and circulation. Should the infant fail to respond to these interventions, advanced resuscitation measures such as intubation and the administration of drugs may be required.
The key components of newborn resuscitation interventions are:
A: Airway
- Position the infant supine with the head in a neutral position.
- Clear the airway (only if obvious signs of obstruction).
- Dry the infant and stimulate the infant to breathe.
- Maintain warmth. Aim to maintain the infant’s temperature between 36.5 and 37.5° degrees C in all non-asphyxiated newborns
Assess the infant’s breathing and heart rate
B: Breathing
- If the infant is not breathing or the heart rate is less than 100 per minute in an infant with poor muscle tone who is breathing ineffectively, then positive pressure ventilation (PPV) is indicated.
- Provide positive pressure ventilation at a rate of 40 – 60 inflations per minute. Aim fo an inspiratory time of 0.3 to 0.5 seconds
- Commence positive pressure ventilation in air (21%) initially for term infants, and air, or up to 30% oxygen for preterm infants who are less than 35 weeks’ gestation.
- Apply a pulse oximeter to the infant’s right hand or wrist.
- Titrate supplemental oxygen administration according to pulse oximetry (wean the oxygen if saturations are above 90%).
- Reassess the infant after 30 seconds of effective positive pressure ventilation.
Reassess the infant’s breathing and heart rate
C: Circulation
- If the heart rate is above 60/min (but below 100/min) continue to provide positive pressure ventilation until the heart rate is above 100/min and the infant is breathing spontaneously and effectively.
- If the heart rate is below 60/min, commence external chest compressions (ECC) and positive pressure ventilation at a ratio of 3:1.
- Increase the FiO2 to 100%.
- Reassess the infant after a further 30 seconds of effective external chest compressions with positive pressure ventilation.
Reassess the infant’s heart rate
- If the heart rate is above 60/min, then external chest compressions can be ceased and positive pressure ventilation continued at 40 – 60 inflations per minute until the heart rate is above 100/min and the infant is breathing effectively.
- If the heart rate is still below 60/min, advanced resuscitation interventions (intravenous access and drug administration) are now indicated.
D: Drugs
- If the heart rate remains below 60/min despite effective ECC with PPV then adrenaline is indicated.
- Volume expanders should be considered if the infant appears shocked and/or blood loss is suspected.
Endotracheal intubation may be considered at several stages, but particularly if positive pressure ventilation with a mask fails to restore an adequate heart rate or the infant does not have a detectable heart rate at birth.
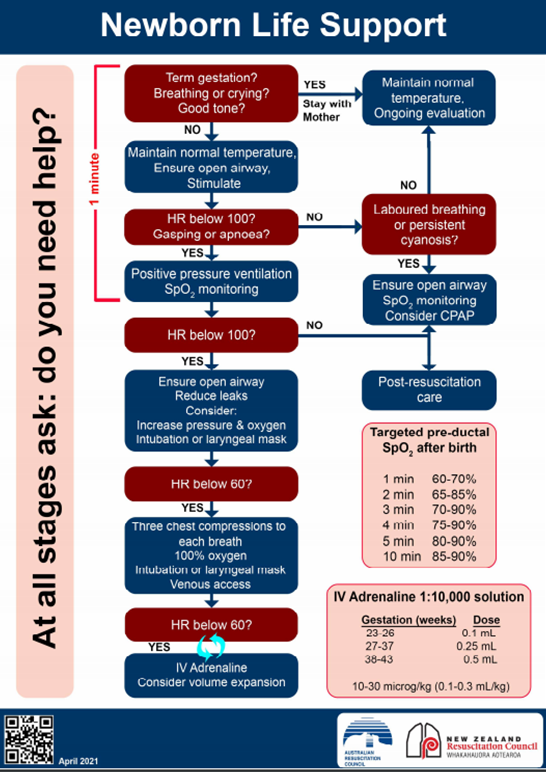
The ANZCOR Newborn Life Support Flow Diagram (2021):
| Key points: The ANZCOR newborn Life Support Flow diagram (2021) continues to focus on the first minute after birth, with an emphasis on rapid assessment and prompt initiation of first response interventions within one minute. Thereafter are no time lines on the flow diagram. This is because it is unrealistic to undertake all of the interventions a newly born infant may require in a set time frame. The key is to continually evaluate the infant’s response to an intervention and move to the next step in the flow diagram if the infant does not respond. It is imperative to ensure that each step is being performed well: i.e. there is no point moving to chest compressions if you have not been providing effective positive pressure ventilation.
Remember: Effective ventilation is the key to successful resuscitation of the newly born infant |
The Australian and New Zealand Council on Resuscitation (ANZCOR) Newborn Life Support flow diagram (April 2021) is provided below, with the interventions relating to Airway, Breathing, Circulation & Drugs shown to the left of the flow diagram. Throughout the resuscitation process, continual reassessment of the infant’s breathing and heart rate primarily determine the subsequent interventions.
|
|

Scan the QR code to download a copy of the ANZCOR Newborn Life Support Flow Chart – April 2021
| Previous | Next |